This gallery, in two parts, A: X-ray therapy and B: Gamma-ray therapy, was prepared by Colin Orton and Peter Almond based, in part, on their presentations at the History Committee Symposium presented at the 2013 AAPM Annual Meeting:
Wilhelm Conrad Röntgen discovered x rays on November 8, 1895.
Because it was quickly realized that the new rays were causing skin damage to those handling the x-ray tubes and hence were, presumably, damaging skin cells, it was theorized that they might be able to kill cancer cells.
Within months, x rays began to be used to treat cancer.
Emile Grubbé
A02
1st use of x rays for cancer radiotherapy.
On January 29, 1896, Emile Grubbé, a medical student in Chicago, who had established a small business making x-ray tubes, initiated a course of treatment on a Mrs. Rose Lee, who had breast cancer.
He delivered 18 daily “one-hour” treatments with the breast in contact with the x-ray tube.
Treatments were terminated when the patient developed excessive skin damage.
This patient died within one month due to systemic disease before local control could be studied.
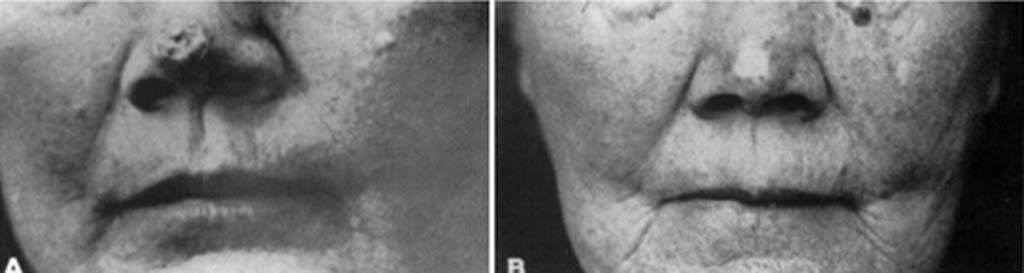
(left) Patient before treatment, (right) Patient 30 years later
A03
The 1st documented successful treatment of a cancer.
In 1899, Thor Stenbeck, in Sweden, treated a basal cell carcinoma on the nose of a patient with 99 x-ray fractions.
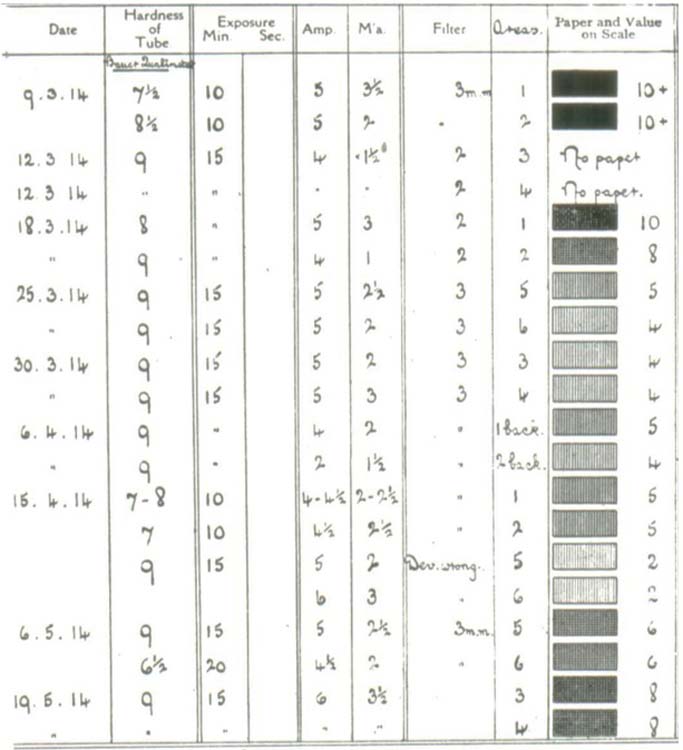
Record of 20 treatments delivered to a patient showing that doses ranged from 2 to 10+
A04
Why so many treatments?
This was common practice in the early years of x-ray therapy because:
Dose was unpredictable and you only found out what dose had been delivered after the completion of each session. Clearly, you couldn’t give the full treatment in a single, unpredictable, fraction.
Outputs were very low and to complete the treatment in one fraction would have taken many hours, even days
William D. Coolidge, an engineer at the General Electric Company’s Research Laboratory in Schenectady, NY
A05
William D. Coolidge solved this problem.
It was not until 1914, after the development of the hot-cathode x-ray tube by William D. Coolidge, that the delivery of high, reproducible, doses became possible.
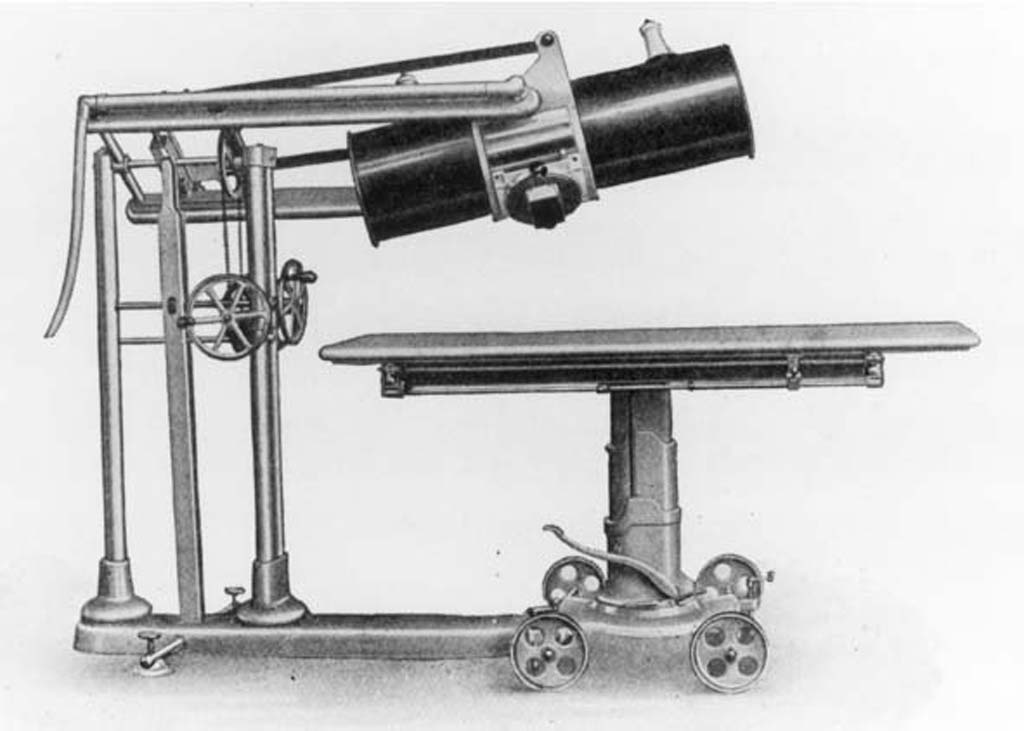
Deep x-ray cannon
A06
The quest for higher energies.
With the advent of the Coolidge x-ray tube came the quest for higher energy x-ray units in order to be able to treat deeper cancers with beams fired from multiple directions, thus reducing the risk of damage to normal tissues and organs surrounding the tumor.
X-ray machines with energies up to about 300 kVp began to be developed.
These were originally called “x-ray cannons” but, later, became known as “orthovoltage” x-ray units.
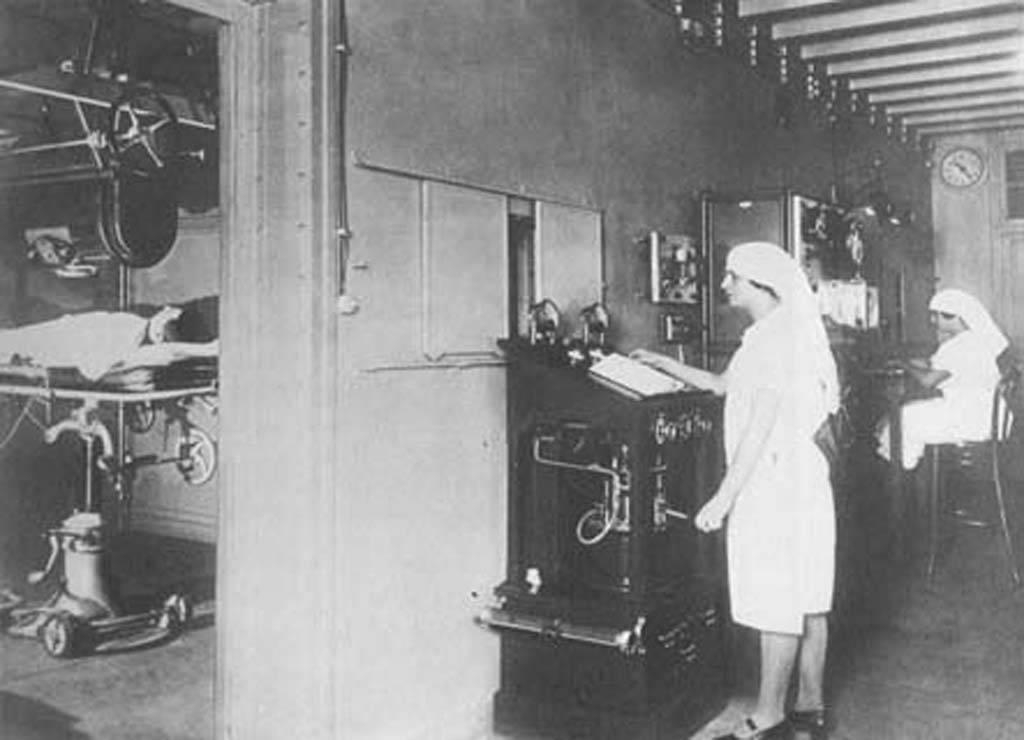
A07
An x-ray cannon facility in Paris in the 1920s.
A08
Development of “supervoltage” x-ray machines.
Between 1930 and 1934 several so-called “supervoltage” x-ray machines were developed in the USA, such as:
A 500 kVp machine installed at Harper Hospital, Detroit
A 600 kVp machine at Caltech
A 750 kVp machine at Memorial Hospital, New York
A 800 kVp machine at Mercy Hospital, Chicago
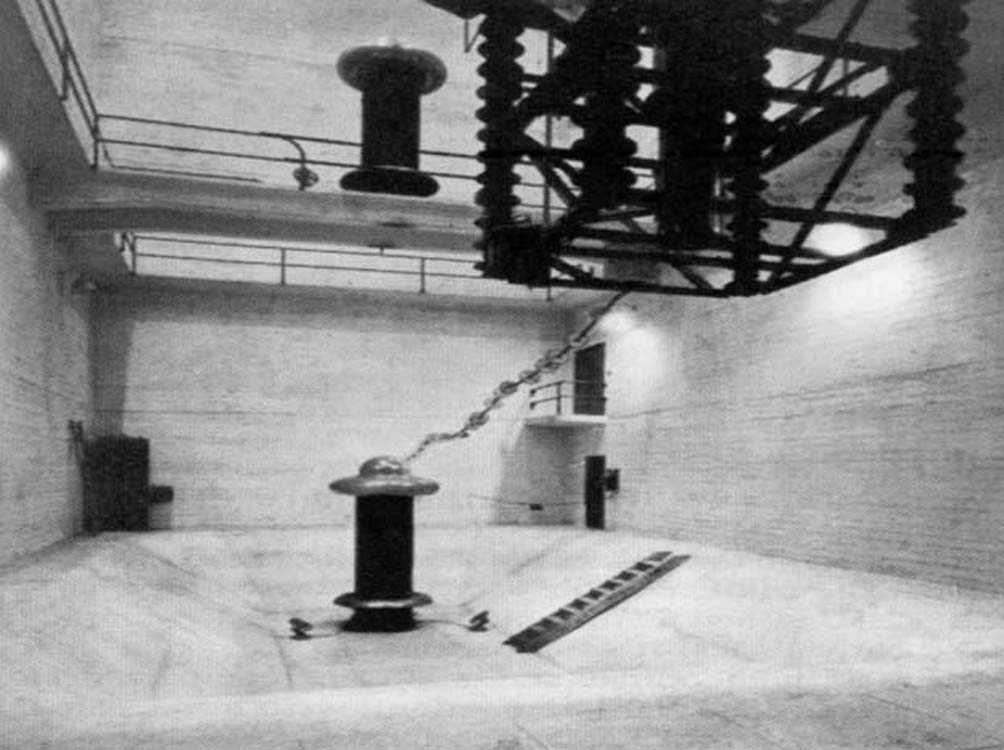
The Caltech 1,000 kVp x-ray machine
A09
1,000 kVp machines.
The World’s 1st 1,000 kVp machines were installed in 1933 at the Swedish Hospital, Seattle, WA, and at Caltech, Pasadena, CA.
The Caltech machine was in a vault 42 m long by 20 m wide by 15 m high.
The 9 m long x-ray tube protruded through the ceiling to the treatment room above.
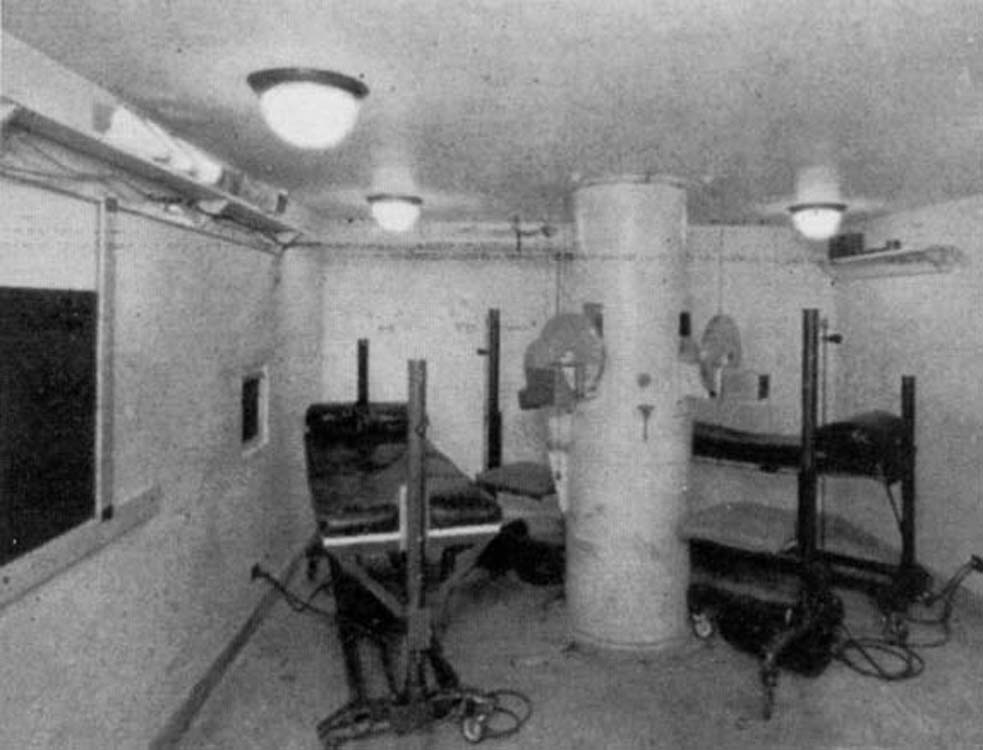
The Caltech treatment room.
A10
The Caltech facility treatment room.
Up to four patients could be treated simultaneously through portals in the central tube.
The St. Bartholomew’s Hospital, London, 1 MVp x-ray machine
A11
St. Bartholomew’s Hospital 1 MVp machine.
A 1 MeV x-ray machine was installed at St. Bartholomew’s Hospital, London, in 1936 by Metropolitan Vickers engineer George Innes.
After installation, he was asked to stay on the staff in order to do measurements on the new machine and to maintain it.
George Innes, de facto, became the medical physicist in charge of the facility, although he was not a physicist by training.
He later became President of the UK Hospital Physicists Association and organized the 1st International Conference on Medical Physics, Harrogate, England in 1965.
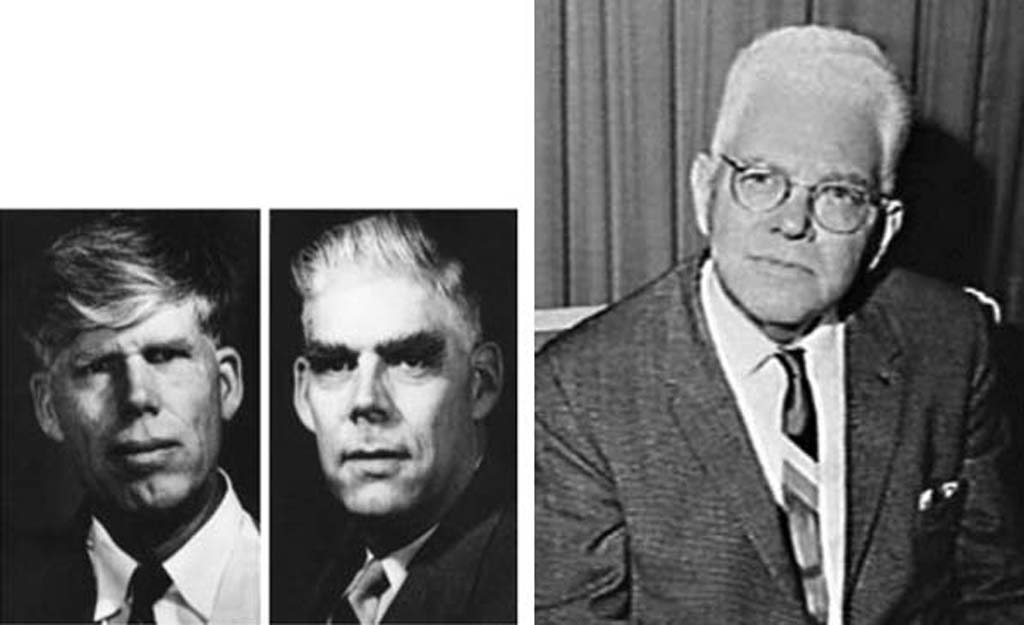
Robert Jemison Van de Graaff
A12
The Van de Graaff generator.
In the late 1920s, Robert Van de Graaff was a Rhodes scholar at Oxford when he conceived the idea for an electrostatic particle accelerator capable of producing very high energies.
By 1931 he was able to produce a potential difference of 1.5 MV with a machine that cost $100 to build!!!
Van de Graaff had increased this to 7 MV by 1933
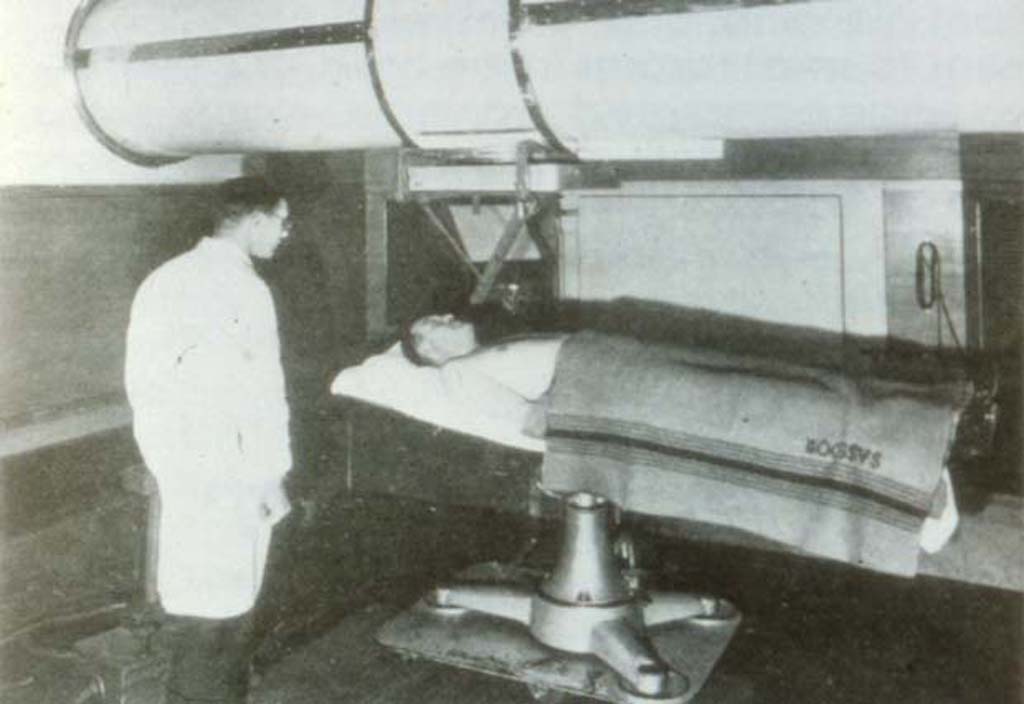
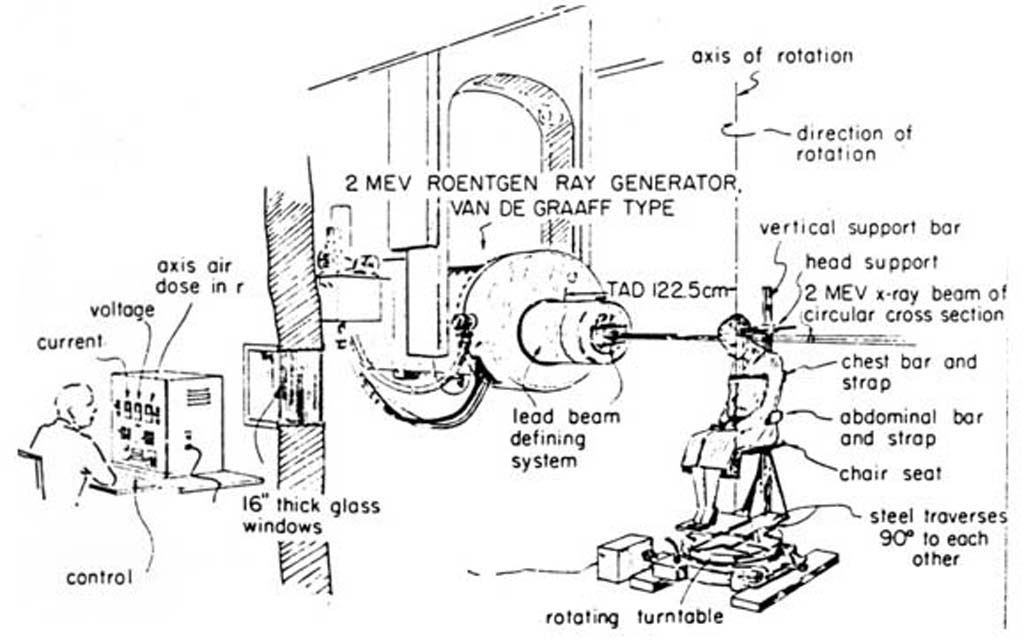
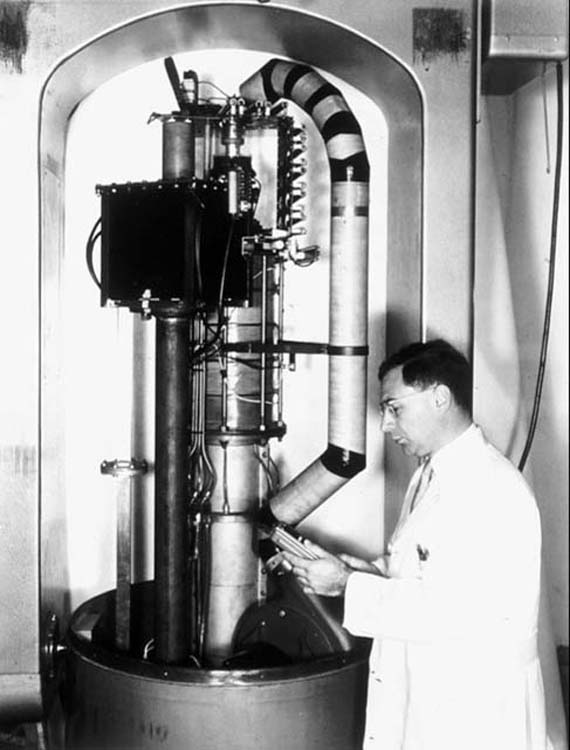
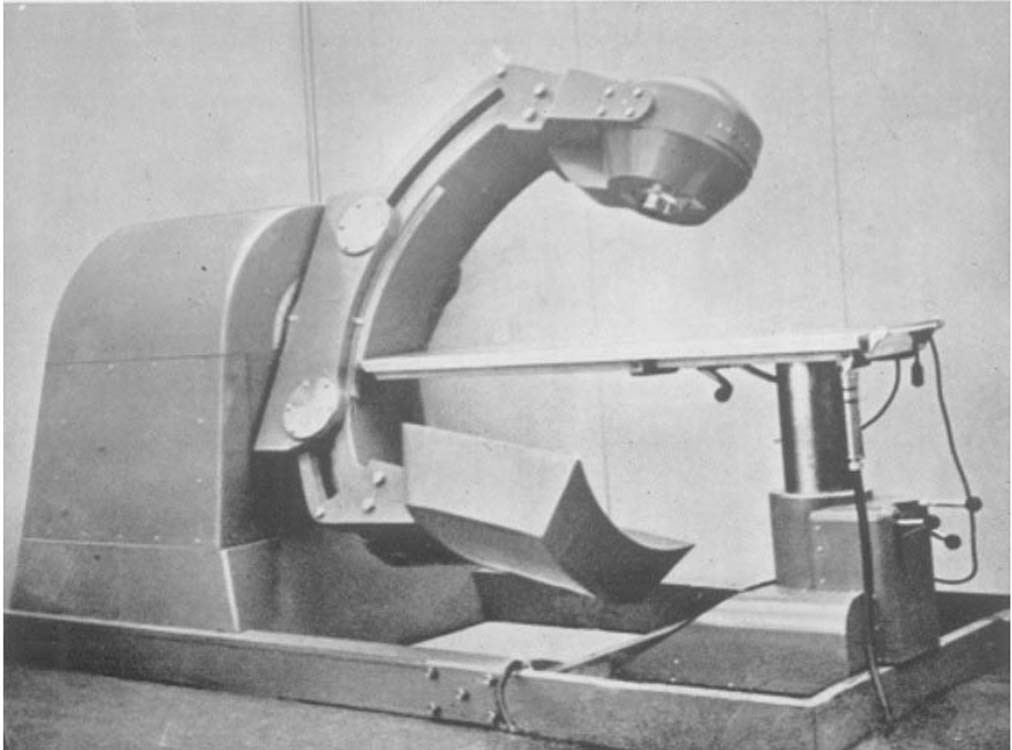
Huntington Memorial Hospital, Boston Van de Graff treatment set up, with the patient sitting on a rotating platform
A13
1st Van de Graaff machine used for radiotherapy.
In 1937, Van de Graaff and John G. Trump (a founding member of the AAPM and uncle of President Donald Trump) installed the first Van de Graaff machine (1 MV air insulated) used for radiotherapy in Huntington Memorial Hospital, Boston.
In 1946, the High Voltage Engineering Corporation, founded by Van de Graaff, began commercial production of a 2-2.5 MV machine.
A total 40 Van de Graaff accelerators were built until their production was discontinued in 1959.
Donald William Kerst: AAPM Honorary Member
A14
1st higher-energy machines.
The quest for even higher energies continued with Donald Kerst, who built the world’s first magnetic induction accelerator at the University of Illinois in 1940.
There was a competition to name it.
“Ausserordentlichhochgeschwindigkeitelektronenentwickelndenschwerarbeitsbeigollitron” was one of the more original entries.
Fortunately, Kerst settled on “betatron”.
Donald Kerst and Gail Adams work on the 22 MeV
A15
Development of the 1st medical betatron.
Several of our famous medical physics pioneers cut their teeth on the University of Illinois betatron: Gail Adams, Lester Skaggs, John Laughlin, and Larry Lanzl.
A16
Smithsonian Institute exhibit.
Donald W. Kerst with the world’s first betatron, built at the University of Illinois in 1940 and now in the Smithsonian Institution.
A17
The betatron in clinical practice.
The betatron had two major problems:
It was very large and would have been difficult to make isocentric.
The x-ray output was low.
Because of these deficiencies, it was soon to be replaced by the linear accelerator.
Russell & Sigurd Varian, and Mark Oliphant
A18
Development of the linear accelerator.
The linear accelerator (linac) grew out of the development of the klystron and the magnetron for the generation of microwaves for radar during the 2nd World War by Russell & Sigurd Varian in Palo Alto, CA, and by Mark Oliphant in Birmingham, England.
Henry Kaplan with an early model of a linac
A19
The 1st Therapy Linac
In the USA, Henry Kaplan realized the potential of linacs for radiotherapy.
He worked with Edward Ginzton to design a medical linac and applied for an NIH grant to construct it, but it was disapproved.
In the UK, the British Atomic Energy Research Establishment designed a medical linac and contracted with the Metropolitan Vickers Electrical Company to build it.
The 1st therapy linac was an 8 MeV stationary machine built by Metropolitan Vickers and installed at Hammersmith Hospital, London, with the 1st patient treated on 19 August, 1953.
The 1st isocentric linac (installed in 1953 in Newcastle, England)
A20
The 1st isocentric therapy linac.
Later in 1953, a 4 MeV isocentric machine was installed by Mullard Research Laboratories at the Newcastle General Hospital, England.
1st patient treated with the 6 MeV linac at Stanford University in 1956
A21
Radiotherapy linacs in the USA.
Edward Ginzton and Bill Hansen worked with the Varian brothers to build a 6 MeV linac, which was installed at Stanford University for Henry Kaplan.
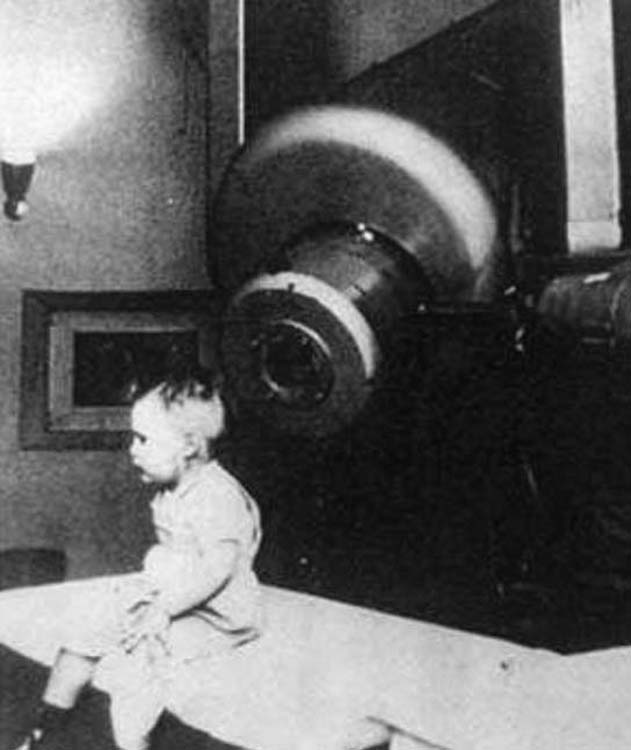
The 1st patient, a 7-month old boy with retinoblastoma, was treated by Dr. Kaplan in January, 1956.
B | Gamma-ray therapy
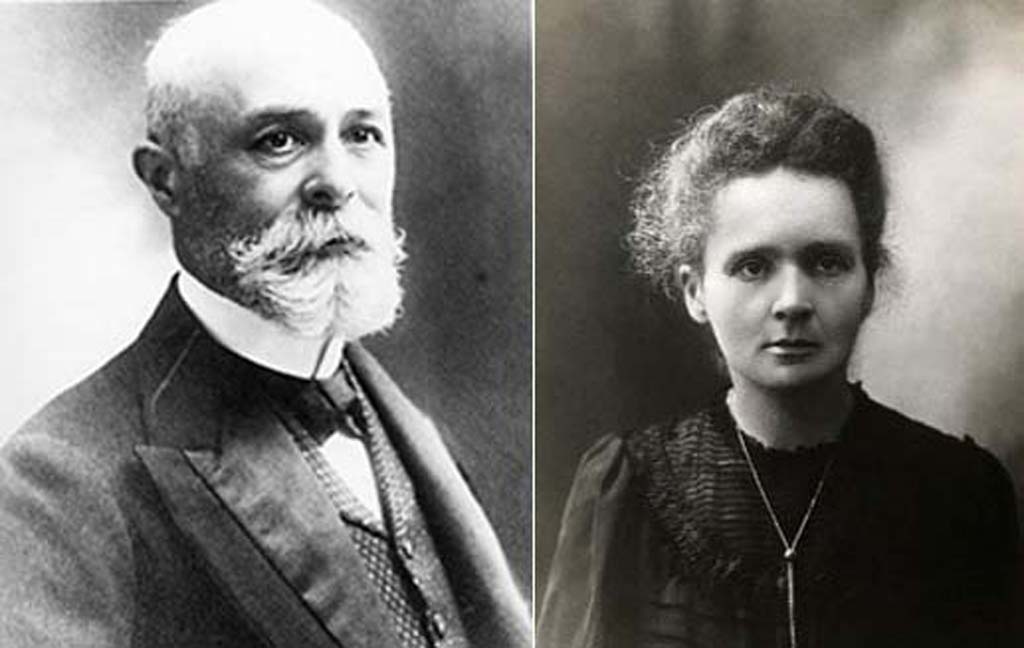
Henri Becquerel and Marie Curie
B01
Discovery of radioactivity and radium.
Henri Becquerel discovered radioactivity in 1896 and radium was discovered by Marie Curie in 1898.
The energy of the gamma rays from radium was about 1 MeV, meaning that they exhibited much better penetration than achieved with early x-ray machines.
Attempts were made between 1915 and 1950 to use these high-energy gamma rays for teletherapy using between 1 and 5 g of radium.
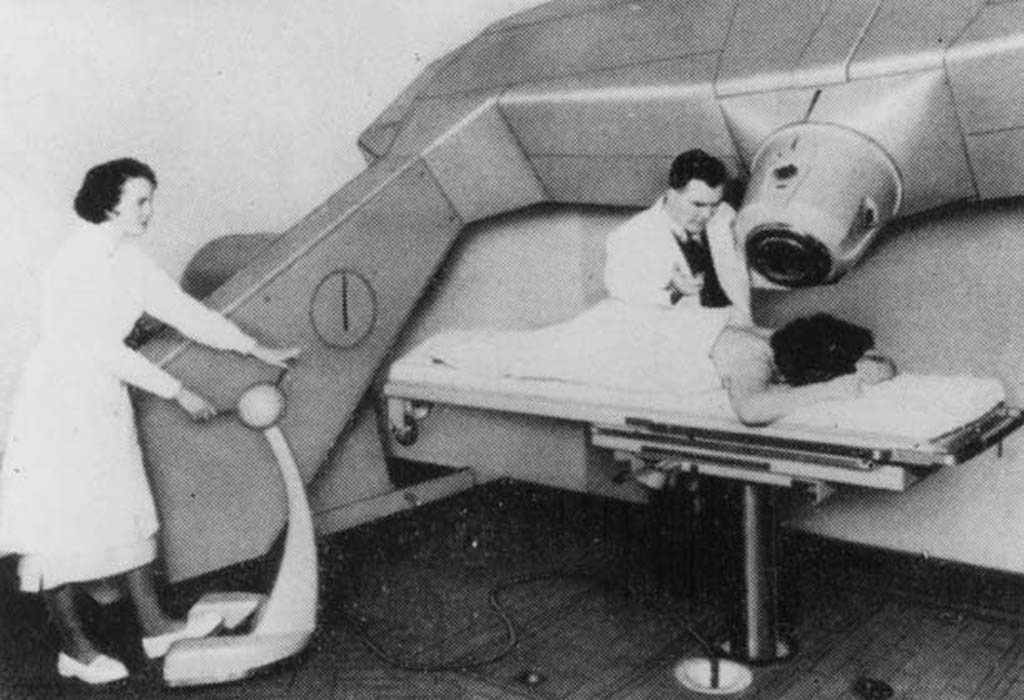
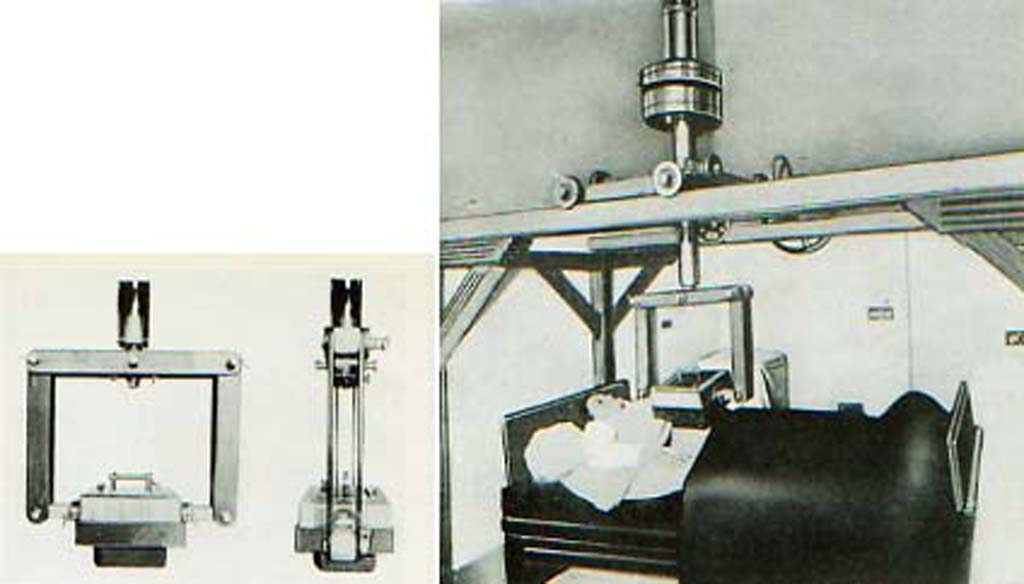
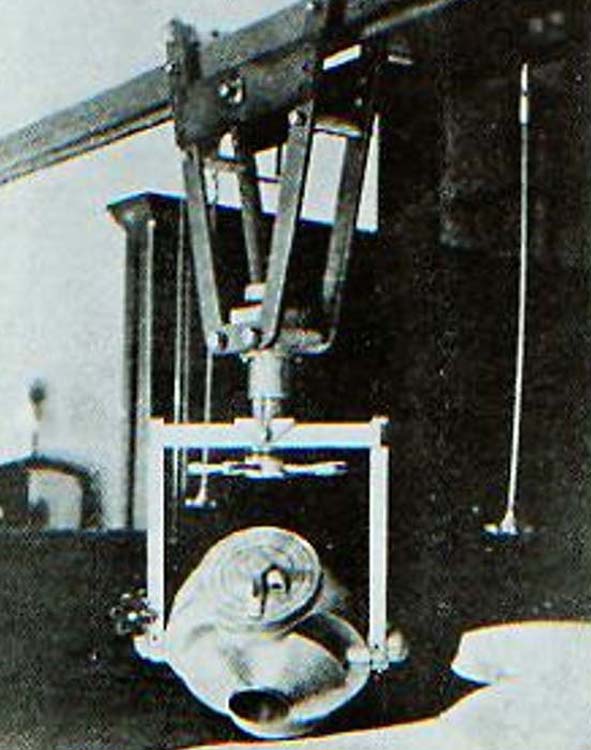
(left) The Paris “radium bomb” with 4 g Ra source. (right) The machine was ceiling mounted and was used at 10 cm SSD
B02
The Paris radium teletherapy unit ca 1926.
With such small amounts of radium available, the dose rates were so low that very short SSDs had to be used and inverse square law fall off of dose greatly reduced the useful depth of penetration.
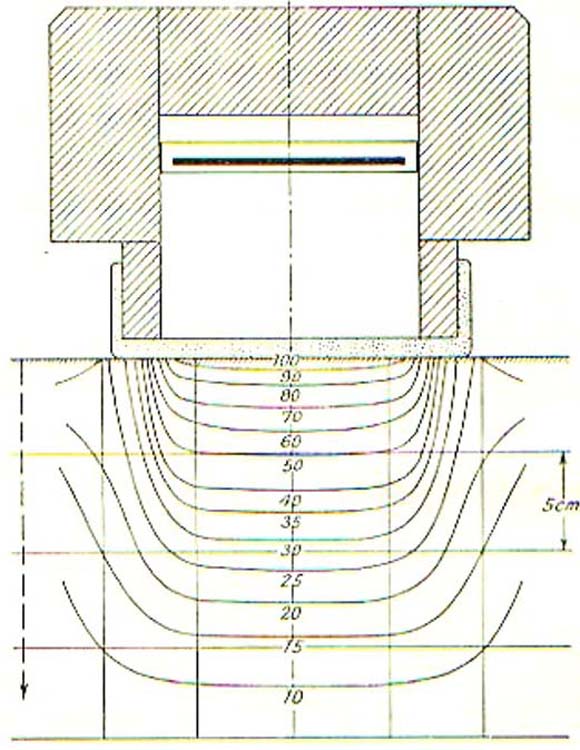
Isodose distribution for the 10 cm SSD Paris “radium bomb”
B03
The penetration was poor.
With the 10 cm SSD of the Paris unit, the depth-dose fell off rapidly, mainly due to inverse-square law.
The Westminster Hospital “radium bomb” (as exhibited at the Science Museum, London)
B04
The 1 g “radium bomb” at the Westminster Hospital, London.
Developed by Ernest Rock Carling, Stanford Cade and Frank Allchin in 1928.
The shutter mechanism was operated by a bicycle brake cable and it was typically operated at about 10 cm SSD.
The 4 g Ra unit at Memorial Hospital, New York
B05
Ra teletherapy in the USA.
In 1928, Gioacchino Failla built a 4 g Ra unit at Memorial Hospital, New York.
This was used at an SSD of 20 cm in order to improve the depth-dose distribution.
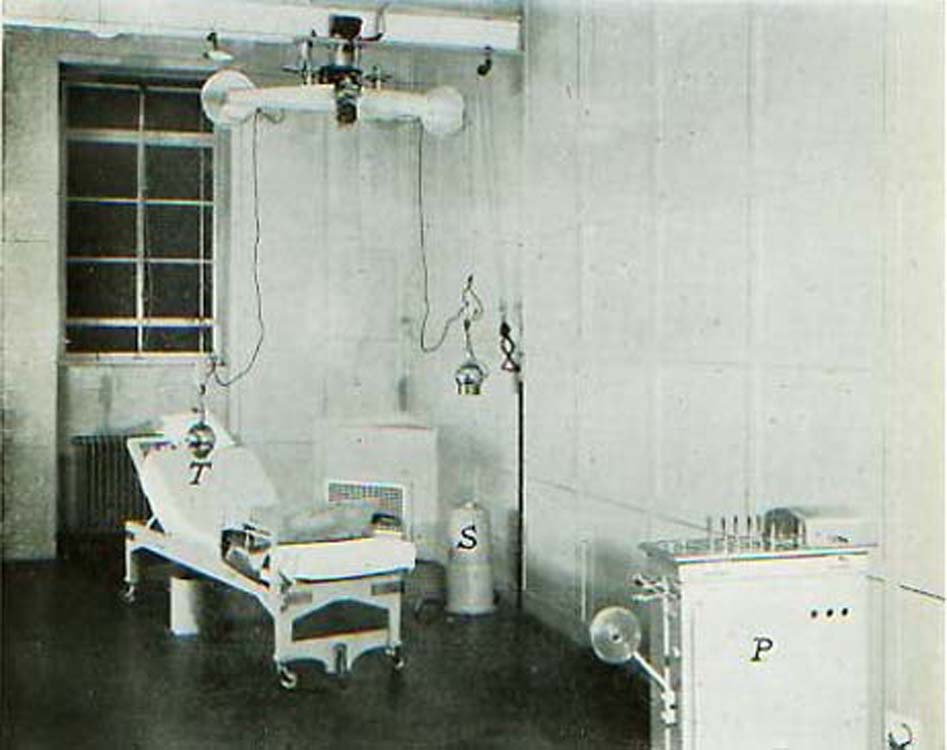
Treatment room for the 4 g Ra teletherapy unit at the Westminster Hospital, London
B06
The 4 g Ra teletherapy unit at the Westminster Hospital, London.
Developed by E. R. Carling, H. Flint, and L. Grimmett in 1930.
Used at 10 cm SSD.
T: treatment couch.
S: source safe.
P: control panel.
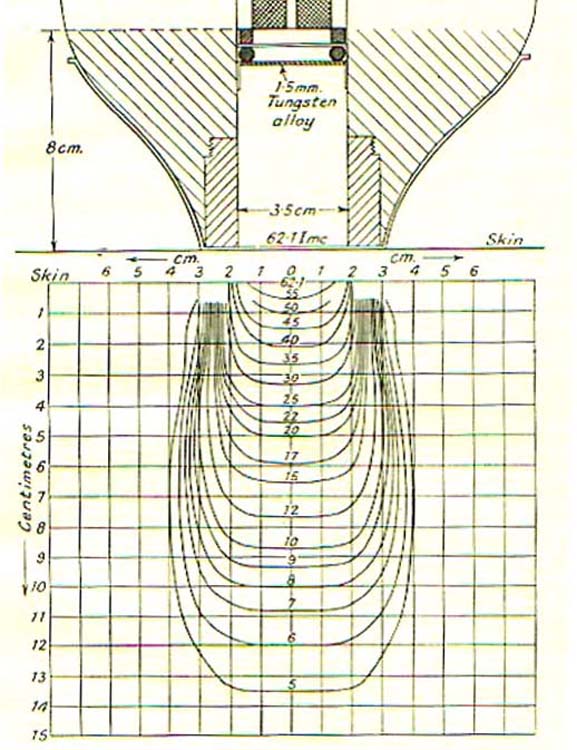
Isodose distribution of the 4 g Westminster Hospital unit with 3.5 cm diameter collimator
B07
Depth-dose distribution for the 4 g Westminster unit.
The collimators on the Westminster Hospital were either 3.5 cm or 9 cm diameter.
Produced relatively sharply defined dose distribution.
Rapid fall off, however, due to short 10 cm SSD.
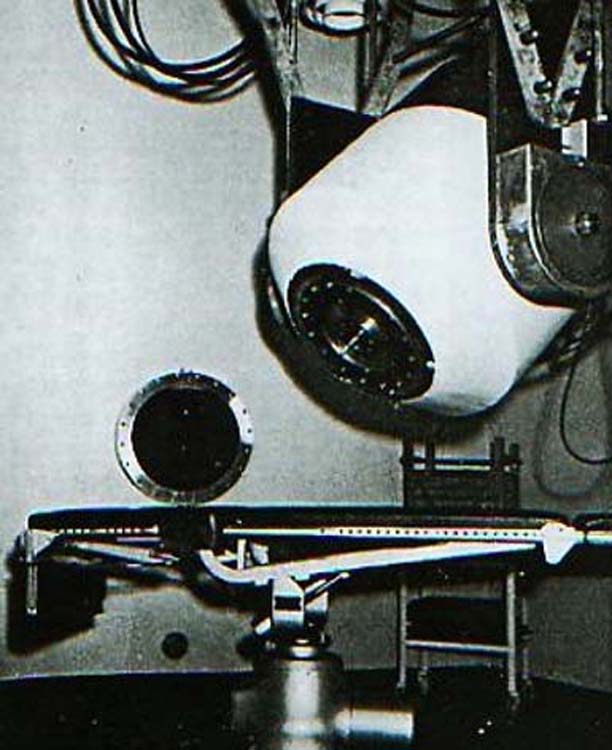
The 50 g Ra unit at Roosevelt Hospital, New York
B08
Longer SSD units.
In order to use longer SSDs to improve the depth-dose distribution, Failla developed a 50 g Ra unit for the Roosevelt Hospital, Janeway Clinic for Therapeutic Radiology, New York, in 1950.
This was used at 25 cm SSD.
A similar unit was installed in Louvain, Belgium
Frédéric and Irène Joliot-Curie
B09
Use of artificially-produced radioactive sources.
In 1934, the French chemists Frédéric and Irène Joliot-Curie produced radioactivity artificially.
Because of the low specific activity, cost and poor availability of radium, only sources in the range 1-50g were possible, which required the use of short SSDs in order to keep treatment times reasonable.
These short SSDs resulted in poor depth-dose characteristics so, in a 1937 paper in Nature on Radium Beam Therapy and High Voltage X-Rays, A. S. Eve and L. G. Grimmett suggested, for the first time, replacing radium with a suitable artificially-produced radionuclide.
By the mid-1940s it began to be realized that the most suitable artificially-produced radionuclides would be Ir-192, Co-60 and Cs-137.
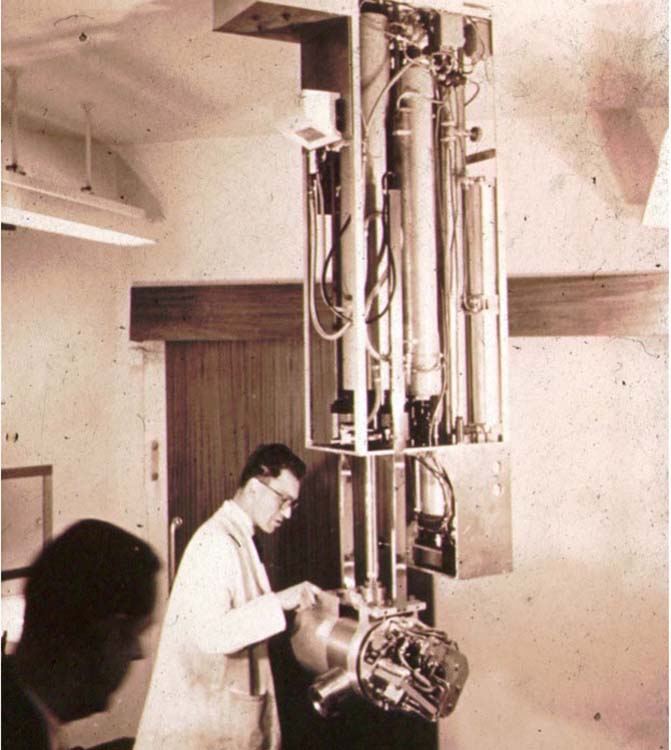
The 1951 Addenbrook’s Hospital Ir-192 teletherapy unit
J.S. Mitchell, a physician/physicist from Cambridge and part of the British scientific contingent at the Atomic Energy Project in Chalk River, Ontario, Canada during and just after the war, had his physicist H. F. Freundlich design an Ir-192 teletherapy unit for him to use at the Radiotherapeutic Centre, Addenbrooke’s Hospital, Cambridge, England.
He treated his 1st patient in June, 1951.
In terms of output this was a good substitute for radium.
With a half-life of just 74 days, however, it required regular source changes and, with the source strengths available at the time, the SSD was just 8 cm, so the depth-dose characteristics were no better than for radium.
Also, with an average gamma-ray energy of about 400 keV compared to 1.2 MeV for Co-60 with its superior depth-dose, it is not surprising that such Ir-192 teletherapy units never caught on.
B11
Co-60 teletherapy.
J.S. Mitchell was the first in print to suggest Co-60 teletherapy in a paper published in the British Journal of Radiology in 1946.
Others soon joined Mitchell in recommending Co-60, including
British physicist William Valentine (Val) Mayneord, who had replaced Mitchell at Chalk River, gave a series of lectures in which he recommended Co-60, including one he presented in 1946 at Toronto General Hospital, which was attended by Harold Johns.
A. J. Cipriani, Chairman of the Biological and Medical Research Branch in Chalk River.
Gilbert Hungerford Fletcher, who was appointed Head of Radiology at the M. D. Anderson Hospital and Tumor Institute in Houston in 1947, having become interested in development of Co-60 teletherapy while serving in the US Army in 1945/46.
Leonard Grimmett, another British physicist, who had been recruited by Gilbert Fletcher to join him at the M.D. Anderson to design and build a Co-60 unit for teletherapy.
Drs. Clark, Bucer, Grimmet, Roy Heflebower (hospital administrator), and Fletcher (L. to R), review plans for their Co-60 unit
B12
The race to build the 1st Co-60 unit.
In the USA, in 1949 Fletcher, Grimmett, and R. Lee Clark, the director of M. D. Anderson, teamed with Marshall Brucer, the research chairman at the Oak Ridge Institute of Nuclear Studies (ORINS), in a joint venture to design and build a Co-60 unit.
B13
Oak Ridge Meeting.
Before the M. D. Anderson team could proceed, however, the AEC wanted a meeting in Washington D.C. in February 1950 to discuss all aspects of cobalt -60 teletherapy.
The meeting was convened February 13, 1950.
There were 33 attendees from the U.S. and Canada, half were radiologists, one third were physicists, and the remainder were from government agencies and industry from both countries.
Chalk River Research Labs. Opened 1945.
B14
Source activation.
It became evident from the meeting that two Co-60 teletherapy units were being constructed in Canada and that it would not be possible to activate a Co-60 source of sufficient specific activity at Oak Ridge for the M. D. Anderson machine and they would have to arrange for a source to be activated at Chalk River, in Canada.
Also, that construction of two Canadian units were well ahead of the Grimmett unit.
In June, 1950, three sources were inserted into the Chalk River reactor for activation, two for the Canadian Co-60 machines and the third for that to be installed at the M. D. Anderson.
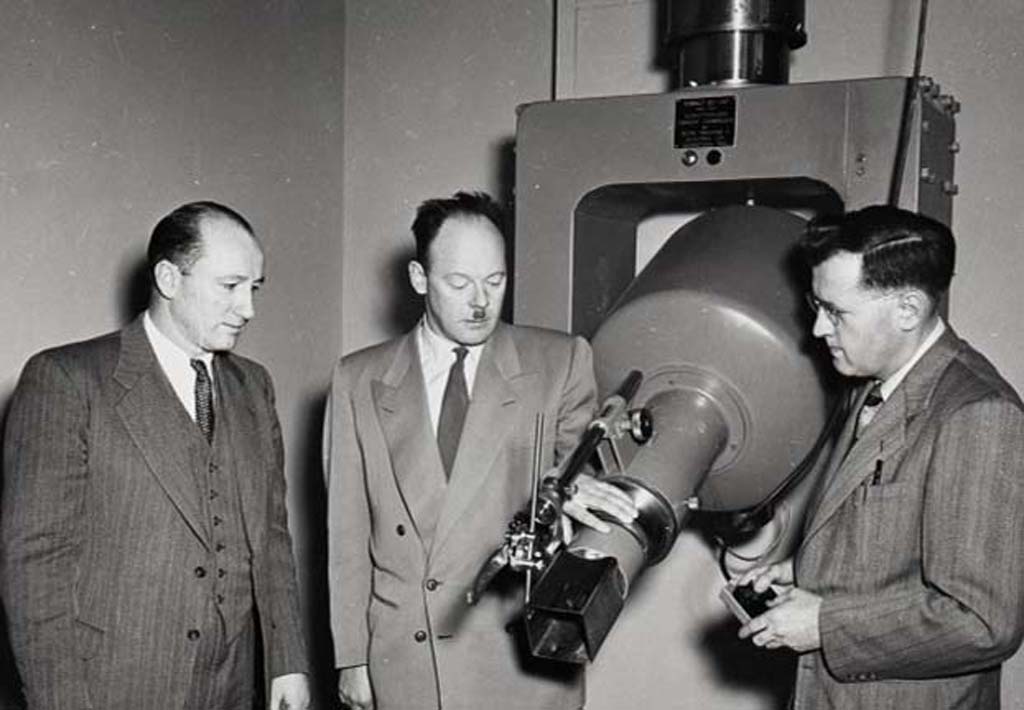
Drs. Fletcher, Brucer, and Dale Trout, General Electric physicist, with the Co-60 unit designed for M.D. Anderson in June 1951
B15
The M. D. Anderson machine.
In October 1950 Grimmett published “A 1,000 Curie Cobalt-60 Irradiator”, in the Texas Reports on Biology and Medicine, the first published paper on a practical Co-60 teletherapy unit.
Construction of the Grimmett-designed M. D. Anderson machine was completed in June, 1951 by General Electric X-Ray Corporation and shipped to Oak Ridge in August, 1951 for installation of the source.
The source, however, did not arrive at Oak Ridge until July, 1952. Too late! The Canadians were already treating patients on their Co-60 units by then.
Due to 14 months of testing at Oak Ridge, combined with delays in the construction of the building to house the unit, the first patient was not treated until February 24, 1954
Note: The first patient treated by Co-60 in the USA was at the Los Angeles Tumor Institute, April 23, 1952 on a home-made unit using multiple smaller Co-60 sources totaling 1080 Ci.
Radiotherapist Thomas Watson, machinist John MacKay, and Harold Johns with the 1st Co-60 unit
B16
The Canadian units.
In Canada, the two sources activated at Chalk River had been commissioned by physicists Harold Johns, to install in a cobalt unit he had designed in the University of Saskatchewan, and Roy Errington and Don Green, to load into a machine designed and built by the Eldorado Mining and Refining Limited, Ottawa, to be installed at the Victoria Hospital, London, Ontario.
The sources were sent out between June and August, 1951.
The Saskatoon source was immediately installed in the Johns unit in August 1951, making this the 1st operational Co-60 machine.
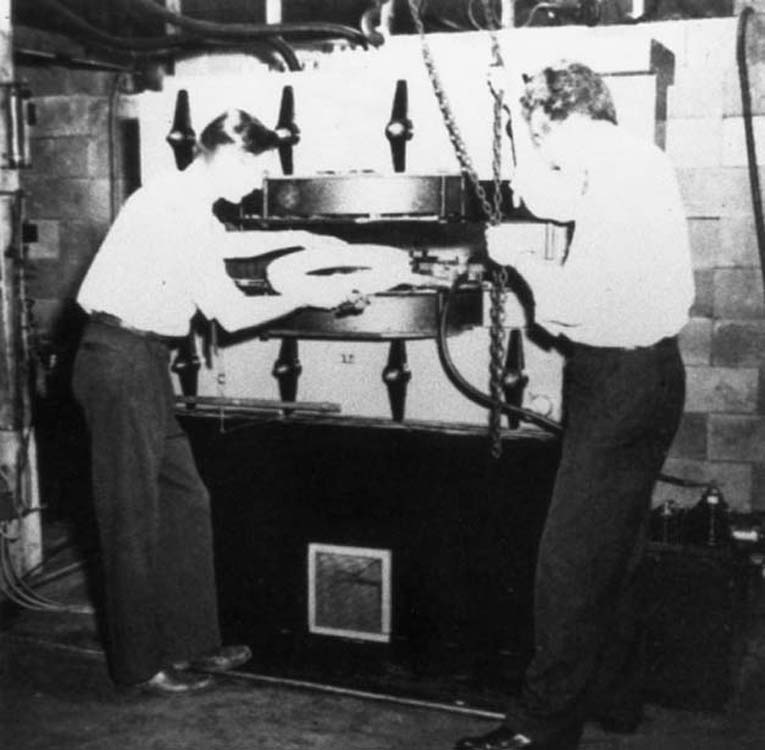
Physicists Silvia Fedoruk and Ed Epp working to commission the 1st Co-60 unit in November 1951
B17
Saskatoon commissioning.
For the next 11 weeks, physicists performed all the measurements to commission the machine for patient treatments and the 1st patient was treated on 8 November, 1951.
The 1st Co-60 unit to treat patients
B18
The Victoria Hospital machine.
Designed by R.F. Errington and D.T. Green, commissioning took less than a week for the Victoria Hospital Co-60 unit and they were able to treat their 1st patient on 27 October 1951, thus making their machine the 1st Co-60 unit to treat patients.
Over the ensuing 40 years, about 35 million cancer patients were treated with Co-60 teletherapy.
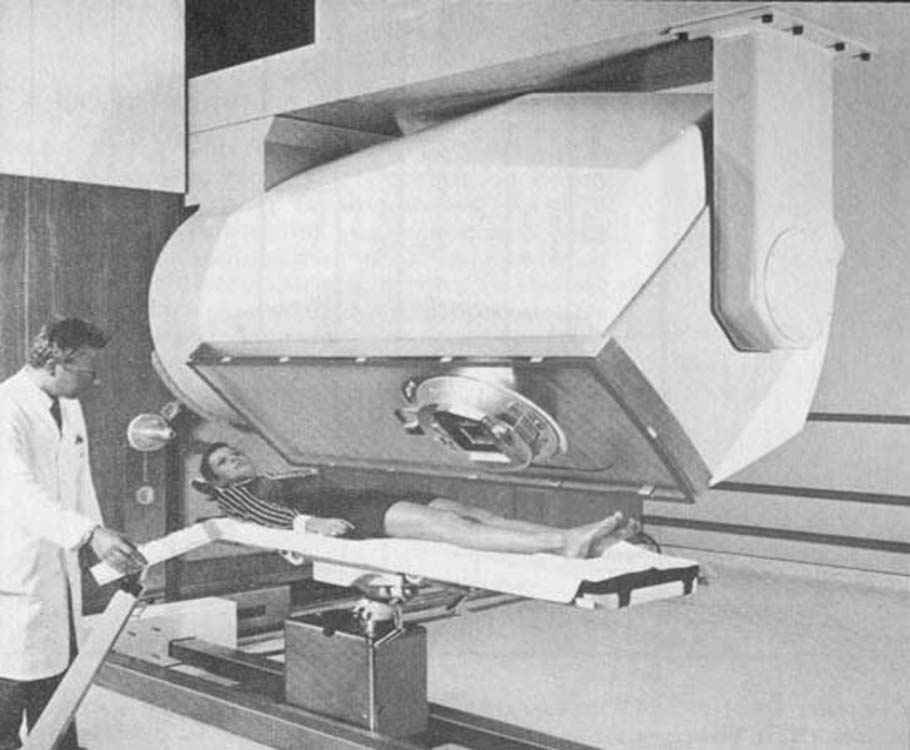
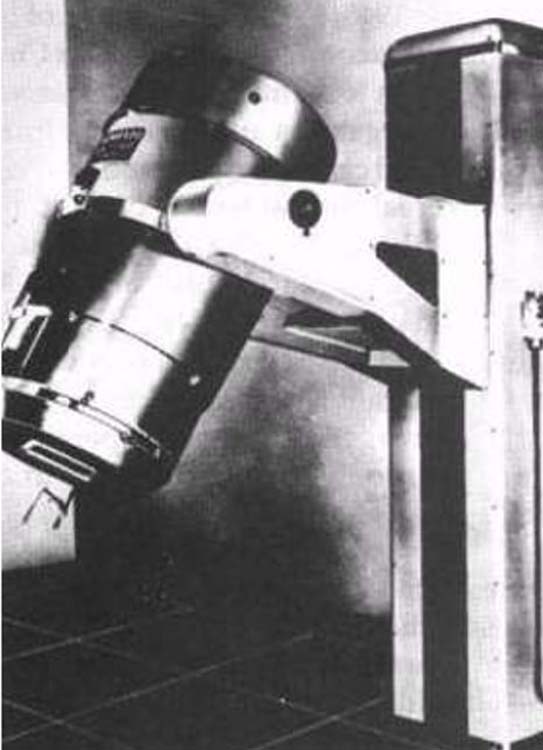
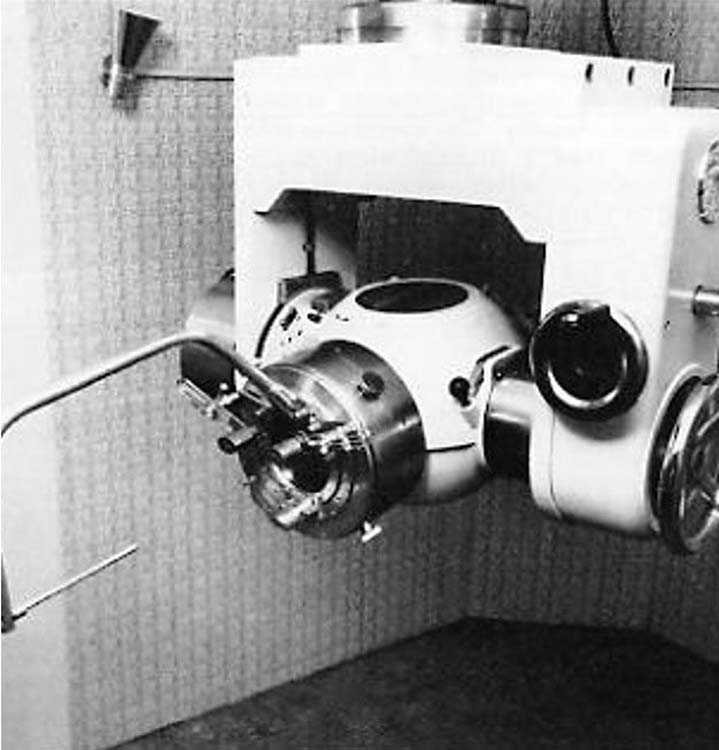
The AECL Theratron isocentric Co-60 unit circa 1953
B19
First commercial Co-60 units.
Atomic Energy of Canada Limited (AECL) took over production of the Eldorado Co-60 units and Johns sold his design for commercial production to Picker X Ray Corporation, Cleveland, Ohio.
In 1953, AECL introduced the 1st isocentric Co-60 unit, the Theratron.
General Electric declined the opportunity to commercialize the Grimmett unit.
For the next 30 years, the number of Co-60 units worldwide dominated the isocentric teletherapy scene until overtaken by linear accelerators.
Physicist Ralph Worsnop with the Guy’s Hospital Cs-137 unit in 1960
B20
Cs-137 teletherapy.
In the early 1950s, Cs-137 began to be extracted from nuclear reactors as a fission fragment and sources suitable for teletherapy became available.
Cs-137 had one advantage over Co-60: its 30-year half-life.
Instead of having to change sources every five years with Co-60 units, they needed to be replaced every 30 years with Cs-137.
There were some disadvantages of Cs-137 teletherapy, however, and only about 400 Cs-137 teletherapy units were ever produced compared with about ten times that number of Co-60 machines.
The 20 – 30 cm SSD Royal Marsden Hospital, London, Cs-137 unit circa 1960
B21
Disadvantages of Cs-137 units.
Disadvantages of Cs-137 when compared with Co-60 included:
Cs-137 sources had a much lower specific activity, so sources had to have a larger diameter (wider penumbra) and had to be used at shorter SSDs, typically 20 – 30 cm.
The gamma-ray energy of about 660 keV was less than the about 1.25 MeV of Co-60, so the depth-dose and skin-sparing characteristics were inferior.
The decay of Cs-137 to Ba-137 produces more electrons per decay and of a higher energy than in the case of Co-60 decay. These electrons became a problem in therapy, producing high skin doses
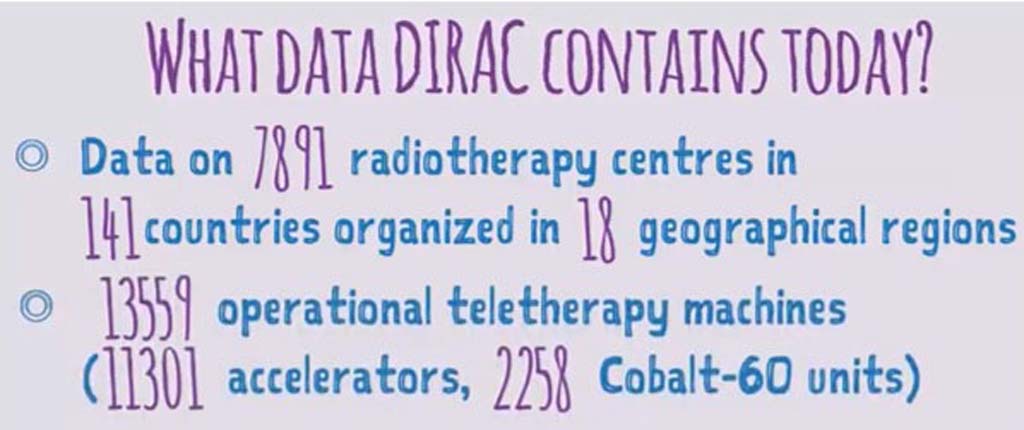
Data from the IAEA Directory of Radiotherapy Centres
B22
The gradual phasing out of artificially-produced radioisotope units.
The Ir-192 and the Cs-137 units were replacements for the tele-radium units and were used at short SSD primarily for head and neck treatment, now much better treated on linacs.
Co-60 units were introduced as replacements for orthovoltage X-ray units and initially represented a significant improvement, but they are gradually being supplanted by higher-energy linacs with better physical characteristics.
In the USA, due to national security concerns about the number of high activity radioactive sources, Federal restrictions have been placed on the use of radioactive teletherapy treatment machines and they have almost all disappeared.
Perhaps the lasting legacy of cobalt-60 units is that the gamma rays became accepted as a standard beam of photons for calibration purposes.