13
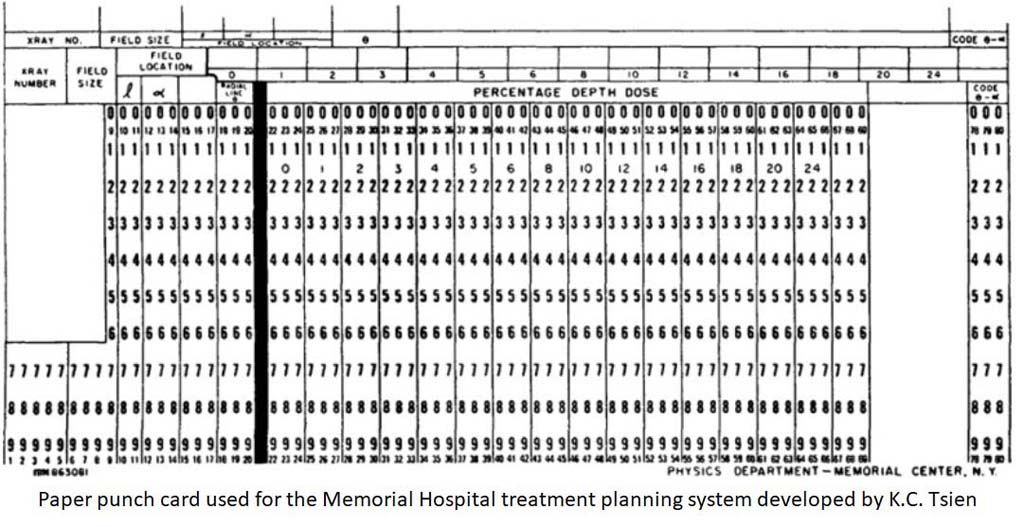

Since most institutions did not have computerized treatment planning, Garrett Holt and colleagues at the Memorial Hospital, New York, built on the K.C. Tsien treatment planning system to develop a Dose Distribution Computation Service for other facilities to use remotely.
Input/output data was transmitted via regular telephone lines to a teletypewriter.

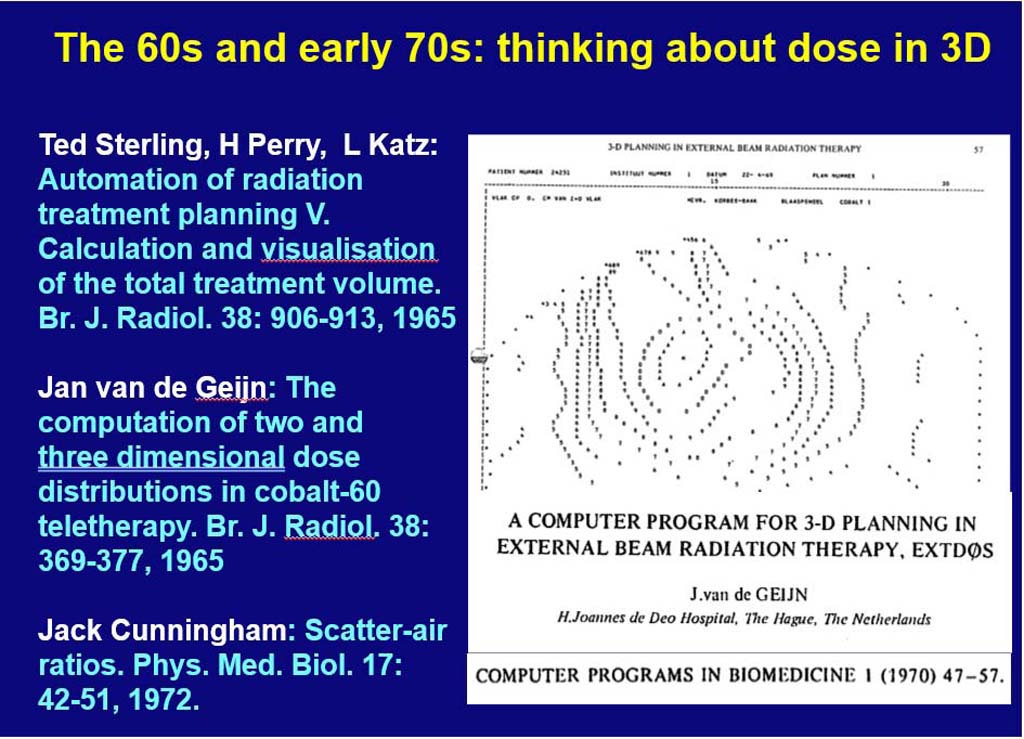
Dan McShan developed one of the 1st 3-D planning systems.
Used interactive color graphics in conjunction with a PDP 11/45 computer.



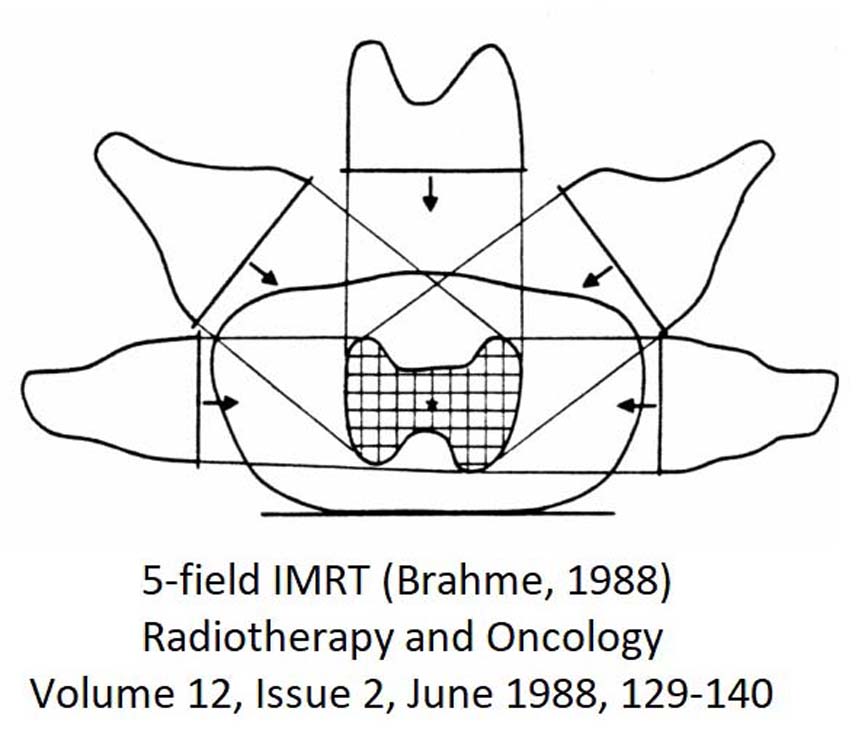


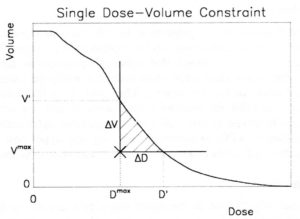
Even with IMRT, a tradeoff has to be found between covering the tumor target volume and sparing the surrounding normal tissues. A method has been developed in the KonRad planning system to add dose-volume constraints for normal organs (cross in lilac (brainstem), green (integral dose) and yellow (left eye)), and to change them interactively during plan optimization.
This method has later been adopted by many planning systems, including Varian Eclipse, Tomotherapy, Oncentra Masterplan, and Dosigray.
Interactive IMRT planning evolved into multi-criteria planning on the Pareto frontier with navigation sliders.