













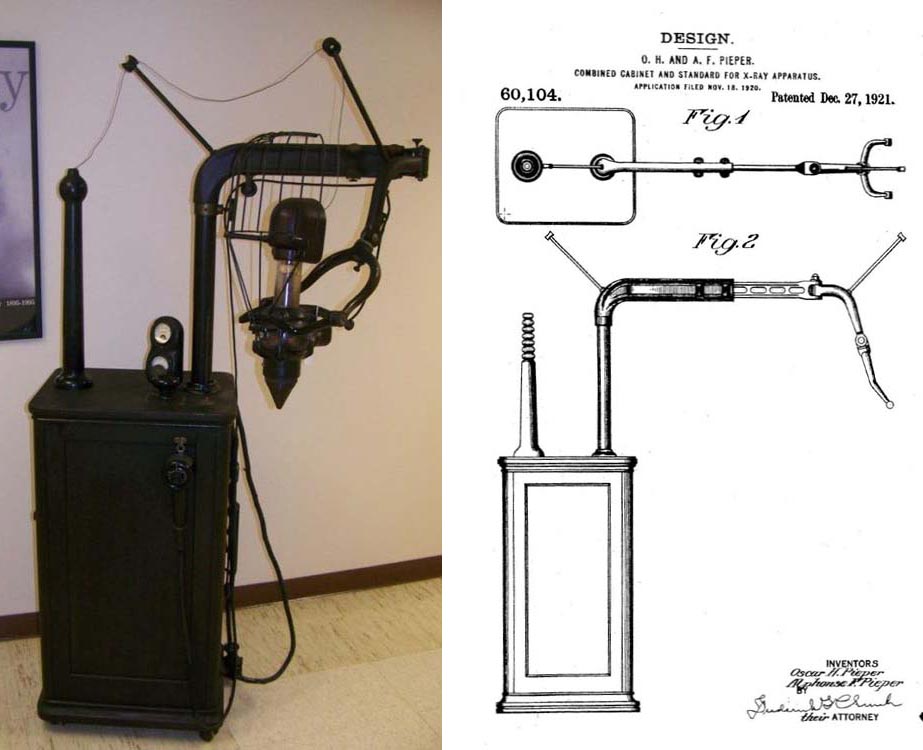
Dental X-Ray machine, manufactured by the Ritter Dental Manufacturing Company, Rochester NY.
Combined cabinet and standard patented by Oscar H. and Alphonse F. Pieper of Rochester, NY on Dec. 27, 1921 (No. 60104). Base cabinet is wood and contains the transformer and tube control mechanism. The X-ray tube is partially shielded by lead glass and enclosed in a wire cage; a spacer cone is on the output port. (Donated by the University of the Pacific, San Francisco, CA)








